Alice Alcorani, Eline Couteau and Chloé Richomme
Mukherjee, R. A. S. (2015). Fetal alcohol spectrum disorders. Paediatrics and Child Health, 25(12), 580–586. doi:10.1016/j.paed.2015.09.008
What is FASD ?
The alcohol consumption by a pregnant mother can lead to five specific diagnostic terms, forming the Fetal Alcohol Spectrum Disorders (FASD) :
- FAS = Fetal Alcohol Syndrome
- Partial FAS
- ARND = Alcohol-related neurodevelopment disorder
- ARBD = Alcohol-related birth defects
We know today that the alcohol consumption during pregnancy can lead to more effects than just the physical stigmata. In fact, it can also lead to growth and brain disorders and to many negative effects for the child development. These effects will be more explained later in this article.
When does alcohol become harmful for an unborn child ?
Is there a safe level of alcohol exposure ? We often consider that high-level exposure results in high risk of harm and low-level exposure results in low risk. However, this question is more complicated and, at this day, the science can’t determine a real “safe level” of consumption. In fact it seems that individual differences in susceptibility to alcohol exposure exist. It means that a high level exposure can have no consequence on his development while a low level exposure in another child can be harmful. Since this individual susceptibility exists, the only safe behaviour to avoid risks of alcohol spectrum disorders is abstinence.
How to diagnose?
At birth, it’s possible to diagnose a FAS within the evidence of an antenatal alcohol exposure, neurological damages, facial stigmata and growth deficits. Other diagnoses can be made during the first year of life if signs and symptoms exist (often cognitive symptoms).
But the diagnosis of a FASD requires to be careful. Indeed, it is essential to investigate and exclude other risk factors, especially when the physical characteristics are absent. It is necessary, among others, to:
- eliminate other genetic factors that may cause neurodevelopmental disorders;
- rule out a potential prematurity, perinatal trauma or postnatal neglect;
- exclude the effects of pharmacological treatments, such as teratogens (which can cause malformations in children), of illicit drugs or tobacco smoking.
For example, it is possible to distinguish disorders due to the consumption of drugs or alcohol depending on the cerebral region affected. In some cases, the disorders can be explained by the association of several of these factors.
Overlapping diagnoses
In the case of FASD, diagnoses often overlap. Thus it is not uncommon to have a person diagnosed with FASD who jointly presents social communication disorders (as in autism) and symptoms of impulsivity (as in attention deficit and hyperactivity disorder). However, the relationship between these three diseases is not always obvious, in FASD the symptoms of impulsivity and communication disorder are due to prenatal alcoholism, unlike the other two developmental pathologies. In addition, these symptoms are not always present in individuals and do not participate in the diagnostic criteria of FASD.
What are the physical stigmata?
Physically, the FASD can be observed on the child’s face (see Figure 1), with: thin upper lip, indistinct philtrum, short palpebral fissures (i.e. opening of the eyelids, characterized by small eyes). But we also find other physical characteristics (less common in some populations) as: on the hand a transverse flexion crease of the palm close to the fingers (“hockey stick palmar creases”) and an underdeveloped upper part of the ear (“railroad track ears” appearance) (see Figure 2). In addition, there are some physical health problems: cardiac, renal, urogenital, gastrointestinal, etc.

Figure 1 Face of child with FASD taken from https://sites.duke.edu/fasd/chapter-1-physical-neuropsychological-and-behavioral-manifestations-of-children-with-fasd/overt-physical-symptoms-of-fas/
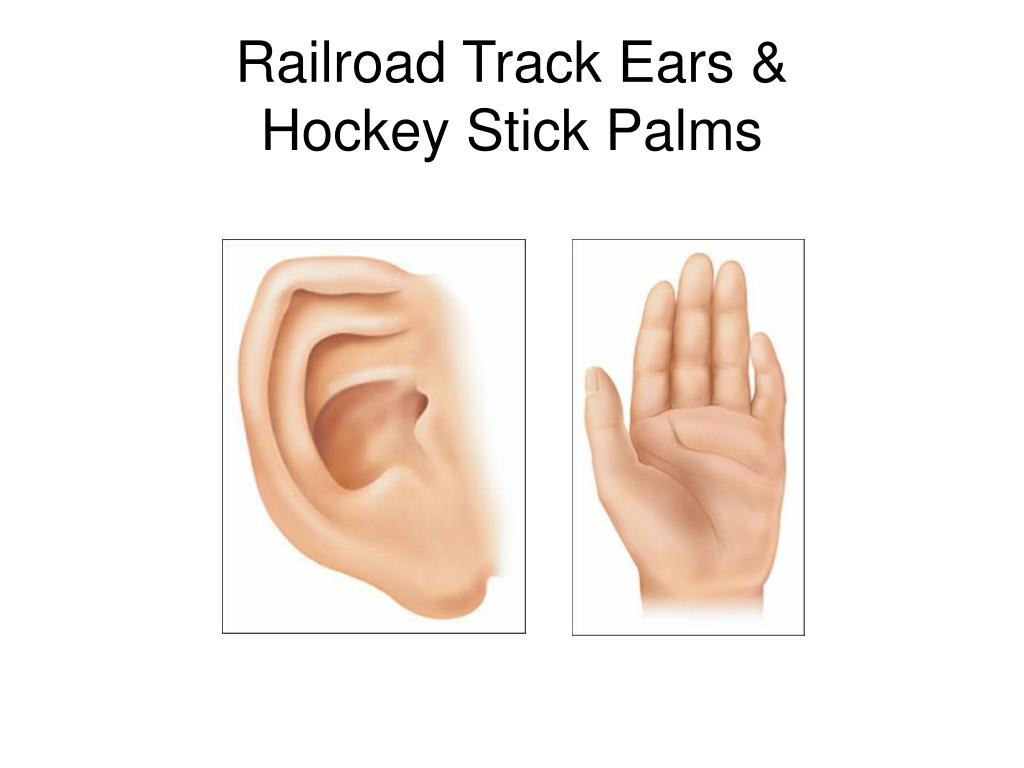
Figure 2 Ear and hand of child with FASD taken from https://fetalalcoholpresentation.weebly.com/what-fas-looks-like.html
What are the cognitive deficits ?
The cognitive deficits associated with FASD are multiple and affect more than one domain.
- Lower IQ;
- Memory (verbal memory)
- Hyperactivity and attention disorder;
- Tiredness
- Social communication problems;
- Processing speed deficits;
- Learning deficits;
- …
These disorders often have repercussions at school and on socialization, in fact FASD children may have important educational difficulties.
What are the behavioural issues ?
Behavioral disorders are very common in FASD. Unfortunately, these are not always well understood and well managed, which alters the patient’s quality of life. Mental health problems (anxiety, mood disorders, schizophrenia, addiction) can occur in these patients when their needs and their cognitive, sensory and communication difficulties are not taken into account. Some studies estimate that 90% of this population would present psychiatric disorders. This results in a loss of self-esteem and a lack of self-confidence that is almost inevitably accompanied by oppositional behavior. A better understanding and management of this disease would be essential to reduce behavioral disorders of people suffering from FASD.
Do we really know FASD ?
International studies have shown that professionals and the general public have a poor level of knowledge of these disorders. Moreover most of our knowledges come from the media instead of scientific articles, leading to conflicting or incomplete informations. Because of this lack of informations, people tend to ignore public health messages and professionals are unable to support the FASD patients and carers.
Management of secondary disabilities
The management of FASD is complex and not optimal. Although some studies are on the subject, research are not numerous, have not yet been able to find a cure for FASD. Moreover, given the heterogeneity of symptoms, it is difficult to implement a treatment that would be effective for the majority of patients.
It also seems complicated to determine a single therapeutic approach for all patients, because of their singularity and the diversity of their symptoms. Thus for some a psychodynamic approach will be preferred while for others a cognitive behavioural therapeutic approach will be more relevant to implement.
A lack of accompaniment can lead to secondary disabilities, which can be very serious. We can find severe mental illnesses leading to criminal and sexually inappropriate behaviors. Studies have suggested that 27% of criminals in Canada have been diagnosed FASD. It is therefore of primary interest to better understand this disease and to be able to provide the necessary support to these poorly supervised patients.
Words we have learned/that can be useful : antenatal (prénatal); neglect (négligence); teratogens (tératogènes); tiredness (fatigabilité); carers (soignants)